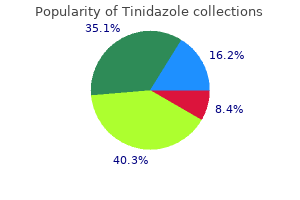
Tinidazole
"Cheap 1000 mg tinidazole visa, antibiotics overdose".
By: S. Gnar, M.B. B.CH. B.A.O., M.B.B.Ch., Ph.D.
Clinical Director, University of Texas Medical Branch School of Medicine
Urine osmolality and urinary electrolytes can be utilized to help distinguish pre renal failure from intrinsic kidney disease (table 5) and might act as one other tool within the evaluation of intravascular volume status antibiotic xanax buy tinidazole. A chest x ray will help assess volume status bacterial conjunctivitis buy 300mg tinidazole fast delivery, however patchy infiltrates may represent pulmonary haemorrhage as seen in certain types of vasculitis antibiotic 875mg 125mg purchase 300mg tinidazole amex. An ultrasound scan will verify that the kidneys are non obstructed virus removal software order tinidazole cheap online, will point out their dimension (small kidneys suggests chronic disease) and should give different clues as to the reason for the renal failure. If however the reason for renal failure continues to be unknown, further investigations are warranted. At this stage involvement of the renal team may be appropriate as the affected person may need a renal biopsy. As a display screen for the reason for the renal disease and in case the affected person is ultimately transferred to the renal unit. The kidney will therefore produce concentrated urine with a low focus of sodium. Hence, if the tubules are intact, less sodium will be excreted in comparison with creatinine (fractional excretion). Sodium retention is increased via stimulation of the renin-angiotensin-aldosterone system; the renal tubules maintain onto more sodium so less is excreted within the urine. Therefore, within the setting of intravascular volume depletion the kidney will produce concentrated urine (excessive osmolality > 500 mosmol/kg) with a low sodium content (< 10-20 mmol/l) � if the tubules are working correctly. Even an adequately stuffed affected person will attempt to retain more water and sodium in times of stress and therefore will produce low sodium, concentrated urine. Academic Department of Critical Care Queen Alexandra Hospital Portsmouth 18 Department of Critical Care Renal Handbook 2014 2. Any urinary biochemistry and osmolality needs to be interpreted with extreme caution if frusemide has been given. A quick guide to urinary sodium and osmolality: Urine Na < 20-30 suggests kidneys retaining Na appropriately Urine osmolality > 500 suggests kidneys concentrating urine appropriately If tubules work � should be 20 times as a lot urea in urine If tubules work � urine osmolality should be a minimum of twice plasma osmolality (if urine osmolality and plasma osmolality comparable � tubules not working) To biopsy or not to biopsy Sometimes from the history and investigations the reason for the renal failure continues to be not recognized and specialist input may be needed. Academic Department of Critical Care Queen Alexandra Hospital Portsmouth Department of Critical Care Renal Handbook 2014 19 Management of the affected person with an acute kidney damage this falls into 5 areas: 1. Decreased venous return additionally results in reduced cardiac operate and hypotension so arterial provide to the kidneys can be compromised. All this is made worse by extrinsic retroperitoneal compression as a result of the increased intra stomach stress. Drug induced interstitial nephritis: Stop the offending drug and contemplate steroids. Obstructive uropathy: Catheterisation for a decrease tract obstruction however nephrostomies may be needed for ureteric obstruction. Ensure that the affected person is nicely hydrated however avoid giving extra fluid � particularly whether it is apparent that the affected person is now not fluid responsive and they stay oliguric or anuric. Once adequately stuffed, if hypotension persists then vasopressor support may be needed. Academic Department of Critical Care Queen Alexandra Hospital Portsmouth Department of Critical Care Renal Handbook 2014 21 Ongoing fluid may be needed if the affected person is polyuric. Management of electrolytes There are a variety of electrolyte disturbances that can be seen, however crucial one acutely is hyperkalaemia. Any potassium supplements for hypokalaemia should be given cautiously Principles of remedy of hyperkalaemia 1. Cardiac safety: antagonise the impact of potassium on excitable cell membranes 2. Treat/appropriate underlying trigger Avoidance of secondary renal insults Further hypotensive events compromise renal perfusion, so limiting (or preventing) renal restoration. Regularly review the drug chart to avoid poisonous unwanted effects to the affected person and to the kidneys. One purpose is because of irregular platelet operate � not their quantity, however how nicely they stick together.
This chapter summarizes the steps to be taken earlier than commencing therapy procedures antibiotic resistance video youtube order tinidazole uk. Radioactive material for analysis or therapy ought to solely be used and saved at medical establishments which have function designed services virus or bacteria tinidazole 1000mg overnight delivery. Licensing necessities differ from country to country and will even embody minimum design and development necessities for the ability antibiotic 24 hours not contagious effective 500 mg tinidazole. Facility design and development the overall rules for the design of nuclear medicine models are mentioned in Chapter three antibiotic quiz pharmacology purchase tinidazole cheap, and additional data relating to therapy models is supplied in Section 6. When designing therapy models, it is important to keep in mind the following: (a) (b) (c) Patients must be housed in a separate room, with dedicated toilet and toilet. Any required shielding must be designed for the proposed floor plan within the eventuality of pregnant patients in adjoining rooms. Close cooperation between the nuclear medicine workers and designers and builders is important. If an current house is to be modified, it could be necessary to determine experimentally the adequacy of walls and floors as radiation shields. If any constructing work is to be carried out, a daily inspection of work in progress is advisable to guarantee adherence to agreed plans and specifications. In particular, it should be famous that: - Brick walls typically have inadequate mortar joints, which is usually a shielding drawback. Responsibilities the physician administering the therapeutic radionuclide dose is finally answerable for taking every precaution to keep away from unnecessary radiation to workers, different patients, guests and the general public. Before commencing therapy, settlement should be reached on medical and radiation security protocols. Training Radionuclide therapy might contain workers exterior the nuclear medicine division, particularly nurses and medical workers. A little effort devoted to familiarization and coaching within the medical and security features of radionuclide therapy can keep away from doubtlessly critical problems later. General rules Radionuclide therapy presents comparatively few hazards to workers and patients, however there are a selection of common rules of radiation security that need to be noticed. This section will think about the requirements for patient accommodation (design necessities together with shielding), as well as radiation security procedures essential for protected practice. For security purposes, every therapy may be divided into different levels, with particular questions of safety which will must be thought of (Table 6. The particular radiation security problem for every of the common therapies is mentioned later on this section. Discharge limits Patients may be discharged solely when the remaining exercise is lower than that prescribed by the local regulatory authority. This may be estimated utilizing a easy ratio of dose charges at a normal distance referenced to the dose rate immediately following dose administration, or by measurement of a dose rate alone. This data is commonly modified to take into account the precise circumstances of each patient. Design of therapy areas There are two types of therapy areas � inpatient areas and areas the place outpatient therapies are administered. The elements to be thought of are: - Types of radiation emitted (photon or particle, or blended); - the potential for contamination and the degree of the hazard; - the kind of waste merchandise generated � human excreta, biological waste and basic waste � and the way in which they should be dealt with; - the function of nursing and medical workers within the care of the patient (high or low level of care). Normally, the one distinction between therapy areas is within the degree of any shielding required and the issues concerned in integrating inpatient areas into a ward, corresponding to entry control and toilet services. Patient comfort should be catered for by radio, music, tv and/or videotape services as well as a comfortable (however easily decontaminated) chair. A floor drain is advisable in case of spillage of the therapy radiopharmaceutical. General inpatient therapy pointers Most inpatient therapies contain 131I, as mirrored within the pointers given beneath. If radiopharmaceuticals with a low risk of contamination are concerned, the guidelines may be suitably modified. No member of workers ought to enter the therapy room without sporting a radiation monitor.
Phase I and pharmacokinetic research of imatinib mesylate in patients with superior malignancies and ranging levels of renal dysfunction: a research of the National Cancer Institute Organ Dysfunction working group bacteria definition for kids buy discount tinidazole. Nephrogenic systemic fibrosis: a gadolinium-associated fibrosing disorder in patient with renal dysfunction antimicrobial jackets buy generic tinidazole 300 mg line. Imatinib remedy length is said to decreased estimated glomerular filtration price in continual myeloid leukemia patients antibiotic resistance marker genes cheap 1000 mg tinidazole fast delivery. Successful remedy of continual myeloid leukemia with imatinib mesylate in a patient with continual renal failure on hemodialysis [letter] infection quality control staff in a sterilization unit of a hospital discount tinidazole 300 mg with mastercard. Acute renal failure secondary to imatinib mesylate remedy in continual myeloid leukemia. Phase I and pharmacokinetic research of imatinib mesylate in patients with superior malignancies and ranging levels of liver dysfunction: a research of the National Cancer Institute Organ Dysfunction working group. Safety and pharmacokinetics of dose-intensive imatinib mesylate plus temozolomide: phase I trial in adults with malignant glioma. Long-time period molecular efficacy and security of imatinib in a patient with continual myeloid leukaemia after renal transplantation [letter]. Imatinib entrance-line therapy is safe and efficient in patients with continual myelogenous leukemia with pre-current liver and/or renal dysfunction. Acute kidney damage presenting a function of leukemic infiltration during therapy for continual myelogenous leukemia. Pharmacokinetics of intravenous imipenem/cilastatin during intermittent haemofiltration. Multiple-dose research of imipenem/cilastatin in patients with end-stage renal illness undergoing long-time period hemodialysis. Pharmacokinetics and pharmacodynamics of imipenem during steady renal replacement therapy in critically sick patients. Single-dose kinetics of imipenem/cilastatin during steady arteriovenous haemofiltration in intensive care patients. Pharmacokinetic profiles of intravenous imipenem/cilastatin during gradual hemodialysis in critically sick patients. A serial software research on twice daily dose of imipenem/cilastatin in patients undergoing gradual hemodialysis [letter]. Steady-state pharmacokinetics of intramuscular imipenem-cilastatin in elderly patients with numerous levels of renal operate. Pharmacokinetics of imipenem-cilastatin in patients with renal insufficiency undergoing steady ambulatory peritoneal dialysis. Pharmacokinetics of imipenem-cilastatin in critically sick patients undergoing steady venovenous hemofiltration. Pharmacokinetics and tolerance after repeated doses of imipenem/cilastatin in patients with extreme renal failure. The pharmacokinetics of imipenem (thienamycin-formamidine) and the renal dehydropeptidase inhibitor cilastatin sodium in regular topics and patients with renal failure. Clinical efficacy, security, and pharmacokinetics of indapamide in renal impairment. A multicenter research of indapamide in hypertensive patients with impaired renal operate. Effect of indapamide on quantity-dependent hypertension, renal haemodynamics, solute excretion and proximal Nephron fractional reabsorption in the canine. Effect of indapamide on the renin-aldosterone system, and urinary excretion of potassium and calcium in important hypertension. Cardiovascular results of indapamide in hypertensive patients with or without renal failure: a dose�response curve. Comparison of the effects of indapamide and hydrochlorothiazide on creatinine clearance in patients with impaired real operate and hypertension. Indapamide is superior to thiazide in the preservation of renal operate in patients with renal insufficiency and systemic hypertension. Effect of indapamide on the renal plasma move, glomerular filtration price and arginine vasopressin in plasma in important hypertension. Indapamide sustained launch: a review of its use in the remedy of hypertension. Identification and pharmacological properties of binding websites for the atypical thiazide diuretic, indapamide. Effects of the acute and continual administration of indapamide on systemic and renal haemodynamics in important hypertension.
Syndromes
- Goiter
- Feelings of restlessness or jitteryness
- You have thoughts of harming yourself or of committing suicide
- Avoid bright lights, TV, and reading during attacks. Rest during severe episodes, and slowly increase your activity.
- Partial (focal) seizure
- Changes in taste or smell
- Severe intellectual disability or other neurological problems
At the first well being care degree virus hoaxes 300mg tinidazole for sale, a proactive approach is required that can assist in early detection of the illness antibiotic vs antibacterial cream discount tinidazole 1000mg on line. Hence providing adequate nephrology providers as well as taking measures to obtain a quantum leap in cadaver kidney donation is important for affected population antibiotic resistance debate order tinidazole with a visa. The world burden of persistent illnesses: overcoming impediments to prevention and control virus zero reviews buy tinidazole 1000 mg overnight delivery. Only about 15% of the world populations are receiving hemodialysis worldwide, with about 80% being handled in Europe, North America, and Japan. Only about twenty p.c obtain therapy in one hundred creating nations which make up over 50% of world population, with some proportion of these residing within the poorest nations dying of uremia due primarily to absence of renal replacement therapy. Those identified with the illnesses should be supplied with appropriate training that explains the therapy regimens and the advantages of enterprise therapy. The epidemiology of persistent kidney illness in sub-Saharan Africa: a systematic evaluate and meta-evaluation. Prevalence and burden of persistent kidney illness among the many common population and high-threat teams in Africa: a systematic evaluate. Chronic kidney illness could also be differentially recognized from preeclampsia by serum biomarkers. Chronic kidney illness after acute kidney harm: a systematic evaluate and meta-evaluation. Increased threat of dying and de novo persistent kidney illness following reversible acute kidney harm. Chronic renal illnesses as a public well being downside: epidemiology, social, and economic implications. Guidance for Industry Pharmacokinetics in Patients with Impaired Renal Function - Study Design, Data Analysis, and Impact on Dosing and Labeling U. Although elimination can happen via any of a number of routes, most drugs are cleared by elimination of unchanged drug by the kidney and/or by metabolism within the liver. Although the obvious type of change arising from renal impairment is a decrease in renal excretion, or probably renal metabolism, of a drug or its metabolites, renal impairment has also been associated with other adjustments, similar to adjustments in absorption, hepatic metabolism, plasma protein binding, and drug distribution. An alternative approach could also be used if such approach satisfies the necessities of the relevant statute, regulations, or both. In particular, a study in sufferers with impaired renal function is recommended when the drug or its energetic metabolites exhibit a slender therapeutic index2 and when excretion and/or metabolism happens primarily via renal mechanisms (excretion or metabolism). A study also should be thought-about when a drug or an energetic metabolite displays a mix of high hepatic clearance (relative to hepatic blood circulate) and significant plasma protein binding. In this setting, renal impairment may induce a big enhance within the unbound concentrations after parenteral administration as a result of a decreased plasma protein binding coupled with little or no change within the total clearance (decrease in unbound clearance). Current information means that the next drug properties could justify this approach:! Drug and energetic metabolites with a comparatively broad therapeutic index and which are primarily eliminated via hepatic metabolism or biliary excretion; Gaseous or unstable drug and energetic metabolites which are primarily eliminated via the lungs; Drugs intended just for single-dose administration until clinical concerns dictate otherwise. Controversy exists relating to the impression of extreme renal impairment on hepatic metabolism. For this cause, a renal impairment study is still thought-about desirable for a drug eliminated primarily via hepatic metabolism until it also has a comparatively broad therapeutic index. Patients on dialysis could require greater doses of certain drugs than sufferers with normal renal function. More usually than not, people with considerably impaired renal function are explicitly excluded from participation in these research, although there could also be a sufficient range of function to get hold of an initial estimate of the consequences of decreased renal function. The strategy used in this section describes the essential "full" study design that could possibly be utilized to most drugs whose pharmacodynamics (i. Then, cases are identified for which some elements of the full study design could three be simplified or excluded relying on the properties of the drug and its anticipated use within the goal patient population. Study Participants the control renal function group in this study should optimally be representative of a typical patient population for the drug to be studied. The study may also embody a bunch of topics with greater renal function than the control renal function group (e. It also allows for the likelihood that the actual patient population could embody some folks with greater renal function than the control group. For a number of-dose research, decrease or less frequent doses as renal function decreases could also be necessary to forestall accumulation of drug and 5 metabolites to unsafe levels.
Buy tinidazole on line. The Antibiotic Resistance Crisis - Exploring Ethics.